Image



IMPORTANT SAFETY INFORMATION & INDICATIONS
Serious and sometimes fatal side effects have been reported with CIMZIA, including tuberculosis (TB), bacterial sepsis, invasive fungal infections (such as histoplasmosis), and infections due to other opportunistic pathogens (such as Legionella or Listeria). Patients should be closely monitored for the signs and symptoms of infection during and after treatment with CIMZIA. Lymphoma and other malignancies, some fatal, have been reported in children and adolescent patients treated with TNF blockers, of which CIMZIA is a member.
INDICATIONS
CIMZIA is a tumor necrosis factor (TNF) blocker indicated for:
- Reducing signs and symptoms of Crohn’s disease (CD) and maintaining clinical response in adult patients with moderately to severely active disease who have had an inadequate response to conventional therapy
- Treatment of adults with moderately to severely active rheumatoid arthritis (RA)
- Treatment of active polyarticular juvenile idiopathic arthritis (pJIA) in patients 2 years of age and older
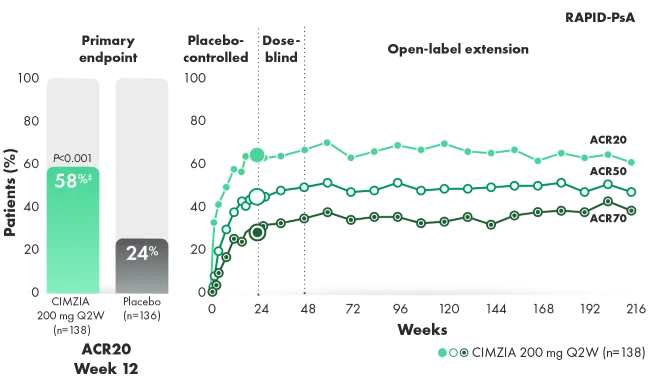
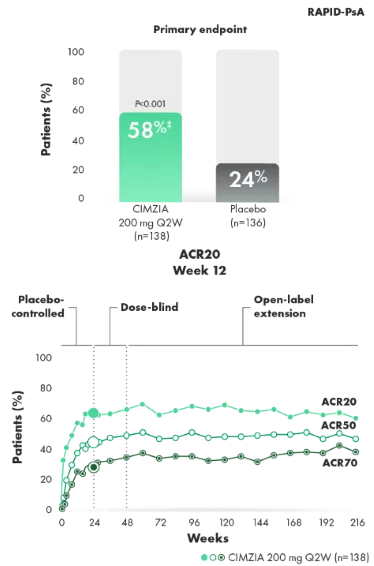
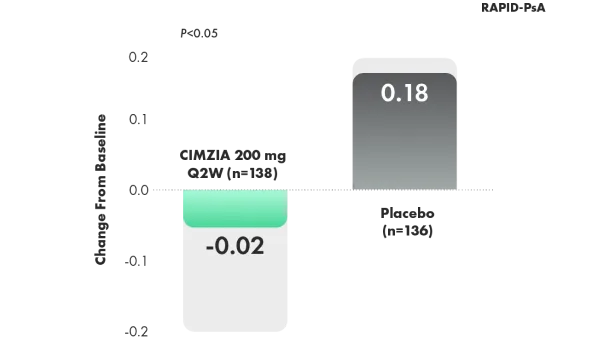
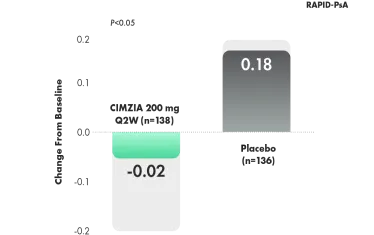
- Treatment of adult patients with active psoriatic arthritis (PsA)
- Treatment of adults with active ankylosing spondylitis (AS)
- Treatment of adults with active non-radiographic axial spondyloarthritis (nr-axSpA) with objective signs of inflammation
- Treatment of adults with moderate-to-severe plaque psoriasis (PSO) who are candidates for systemic therapy or phototherapy
IMPORTANT SAFETY INFORMATION (CONT’D)
CONTRAINDICATIONS
CIMZIA is contraindicated in patients with a history of hypersensitivity reaction to certolizumab pegol or to any of the excipients. Reactions have included angioedema, anaphylaxis, serum sickness, and urticaria.
SERIOUS INFECTIONS
Patients treated with CIMZIA are at increased risk for developing serious infections that may lead to hospitalization or death. Most patients who developed these infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids.
Discontinue CIMZIA if a patient develops a serious infection or sepsis.
Reported infections include:
- Active tuberculosis (TB), including reactivation of latent TB. Patients with TB have frequently presented with disseminated or extrapulmonary disease. Test patients for latent TB before CIMZIA use and during therapy. Initiate treatment for latent TB prior to CIMZIA use.
- Invasive fungal infections, including histoplasmosis, coccidioidomycosis, candidiasis, aspergillosis, blastomycosis, and pneumocystosis. Patients with histoplasmosis or other invasive fungal infections may present with disseminated, rather than localized, disease. Antigen and antibody testing for histoplasmosis may be negative in some patients with active infection. Consider empiric anti-fungal therapy in patients at risk for invasive fungal infections who develop severe systemic illness.
- Bacterial, viral, and other infections due to opportunistic pathogens, including Legionella and Listeria.
Carefully consider the risks and benefits of treatment with CIMZIA prior to initiating therapy in the following patients: with chronic or recurrent infection; who have been exposed to TB; with a history of opportunistic infection; who resided in or traveled in regions where mycoses are endemic; with underlying conditions that may predispose them to infection. Monitor patients closely for the development of signs and symptoms of infection during and after treatment with CIMZIA, including the possible development of TB in patients who tested negative for latent TB infection prior to initiating therapy.
- Do not start CIMZIA during an active infection, including localized infections.
- Patients older than 65 years, patients with co-morbid conditions, and/or patients taking concomitant immunosuppressants may be at greater risk of infection.
- If an infection develops, monitor carefully and initiate appropriate therapy.
MALIGNANCY
Lymphoma and other malignancies, some fatal, have been reported in children and adolescent patients treated with TNF blockers, of which CIMZIA is a member.
- Consider the risks and benefits of CIMZIA treatment prior to initiating or continuing therapy in a patient with known malignancy.
- In clinical trials, more cases of malignancies were observed among CIMZIA-treated patients compared to control patients.
- In CIMZIA clinical trials, there was an approximately 2-fold higher rate of lymphoma than expected in the general U.S. population. Patients with rheumatoid arthritis, particularly those with highly active disease, are at a higher risk of lymphoma than the general population.
- Malignancies, some fatal, have been reported among children, adolescents, and young adults being treated with TNF blockers. Approximately half of the cases were lymphoma, while the rest were other types of malignancies, including rare types associated with immunosuppression and malignancies not usually seen in this patient population.
- Postmarketing cases of hepatosplenic T-cell lymphoma (HSTCL), a rare type of T-cell lymphoma, have been reported in patients treated with TNF blockers, including CIMZIA. These cases have had a very aggressive disease course and have been fatal. The majority of reported TNF blocker cases have occurred in patients with Crohn’s disease or ulcerative colitis, and the majority were in adolescent and young adult males. Almost all of these patients had received treatment with azathioprine or 6-mercaptopurine concomitantly with a TNF blocker at or prior to diagnosis. Carefully assess the risks and benefits of treating with CIMZIA in these patient types.
- Cases of acute and chronic leukemia were reported with TNF blocker use.
HEART FAILURE
- Worsening and new onset congestive heart failure (CHF) have been reported with TNF blockers. Exercise caution and monitor carefully.
HYPERSENSITIVITY
- Angioedema, anaphylaxis, dyspnea, hypotension, rash, serum sickness, and urticaria have been reported following CIMZIA administration. If a serious allergic reaction occurs, stop CIMZIA and institute appropriate therapy. The needle shield inside the removable cap of the CIMZIA prefilled syringe contains a derivative of natural rubber latex that may cause an allergic reaction in individuals sensitive to latex.
HEPATITIS B VIRUS REACTIVATION
- Use of TNF blockers, including CIMZIA, may increase the risk of reactivation of hepatitis B virus (HBV) in patients who are chronic carriers. Some cases have been fatal.
- Test patients for HBV infection before initiating treatment with CIMZIA.
- Exercise caution in patients who are carriers of HBV and monitor them before and during CIMZIA treatment.
- Discontinue CIMZIA and begin antiviral therapy in patients who develop HBV reactivation. Exercise caution when resuming CIMZIA after HBV treatment.
NEUROLOGIC REACTIONS
- TNF blockers, including CIMZIA, have been associated with rare cases of new onset or exacerbation of central nervous system and peripheral demyelinating diseases, including multiple sclerosis, seizure disorder, optic neuritis, peripheral neuropathy, and Guillain-Barré syndrome.
HEMATOLOGIC REACTIONS
- Rare reports of pancytopenia, including aplastic anemia, have been reported with TNF blockers. Medically significant cytopenia has been infrequently reported with CIMZIA.
- Consider stopping CIMZIA if significant hematologic abnormalities occur.
DRUG INTERACTIONS
- Do not use CIMZIA in combination with other biological DMARDs.
AUTOIMMUNITY
- Treatment with CIMZIA may result in the formation of autoantibodies and, rarely, in development of a lupus-like syndrome. Discontinue treatment if symptoms of a lupus-like syndrome develop.
IMMUNIZATIONS
- Avoid use of live vaccines during or immediately prior to initiating CIMZIA. Update immunizations in agreement with current immunization guidelines prior to initiating CIMZIA therapy.
ADVERSE REACTIONS
- The most common adverse reactions in CIMZIA clinical trials (≥8%) were upper respiratory infections (18%), rash (9%), and urinary tract infections (8%).
Please refer to full Prescribing Information.
US-CZ-2400612